COMPOSITE IMAGE BY JEROME CRISTOBAL FROM INQUIRER STOCK PHOTOS
(First of two parts)
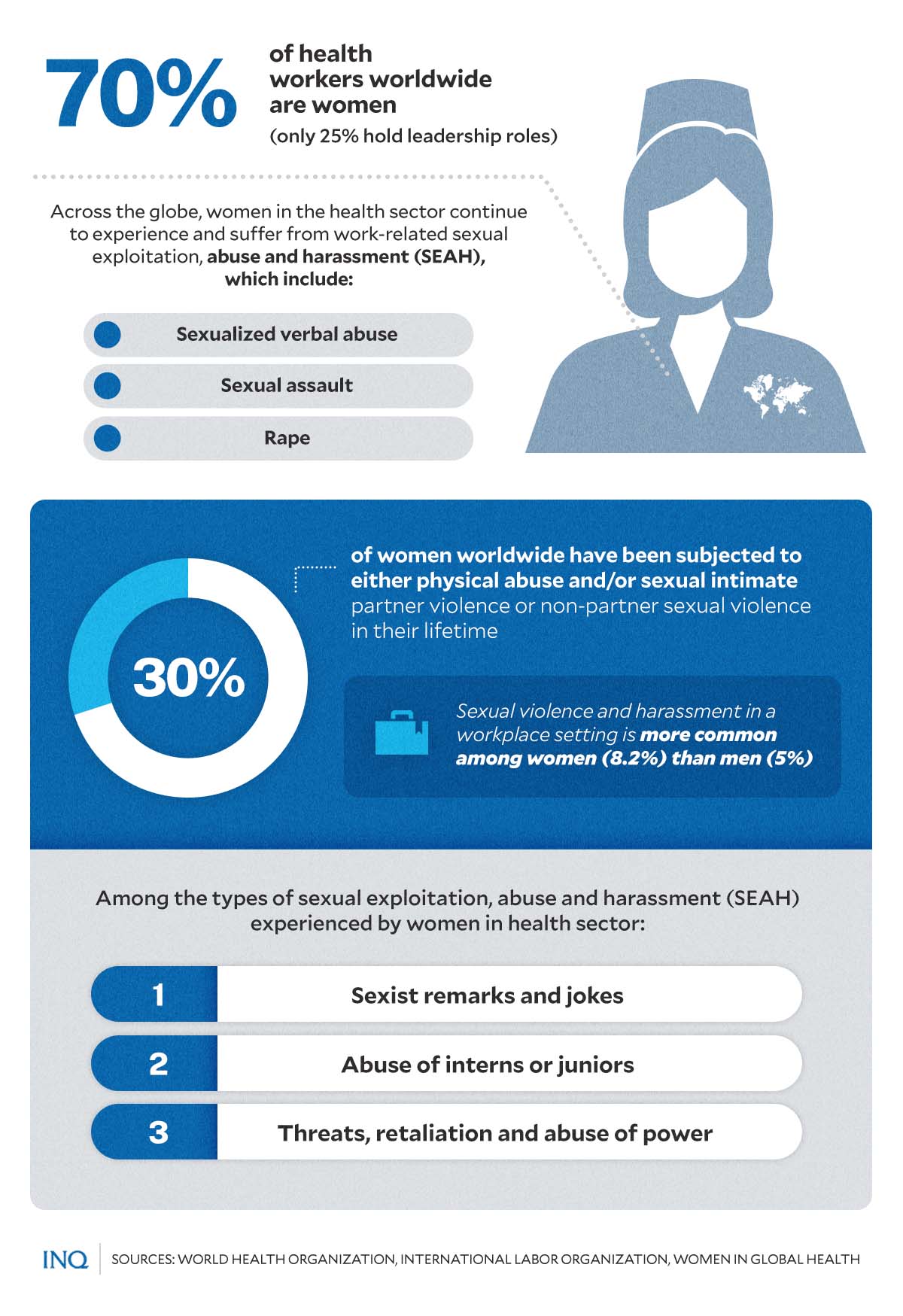
MANILA, Philippines—Women form 70 percent of workers in the health sector worldwide.
But despite the improvement in the representation of women in the most highly-paid occupations and the acknowledgment of their exceptional contribution to health service delivery, many women health workers suffer from workplace violence and harassment.
According to World Health Organization (WHO), 30 percent of women worldwide have been subjected to either physical abuse or sexual violence by partners or non-partners.
Unfortunately, the cases of abuse against women do not stop in households.
Data from a joint analysis by the International Labour Organization, Lloyd’s Register Foundation (LRF), and analytics company Gallup said violence and harassment at work remain widespread globally.
GRAPHIC Ed Lustan
Women (23.2 percent) are slightly more likely than men (22.4 percent) to fall victim to workplace violence and harassment over their working life.
Women were also more exposed to psychological and sexual violence and harassment at work (18.6 percent and 8.2 percent) than men (17.3 percent and 5 percent).
READ: ‘Widespread phenomenon’: Workplace violence, harassment
A recently published policy report titled “Her Stories: Ending Sexual Exploitation, Abuse and Harassment of Women Health Workers” by the non-governmental organization (NGO) Women in Global Health (WGH) delved into cases of sexual exploitation, abuse and harassment (SEAH) experienced by women in the health sector.
“[B]ehind the apparent respect paid to the women who deliver health services to around 5 billion people globally, is a dark story that often remains untold—significant numbers of women health workers experience violence and harassment in the course of their work,” the report noted.
SEAH: ‘Serious, widespread, preventable’
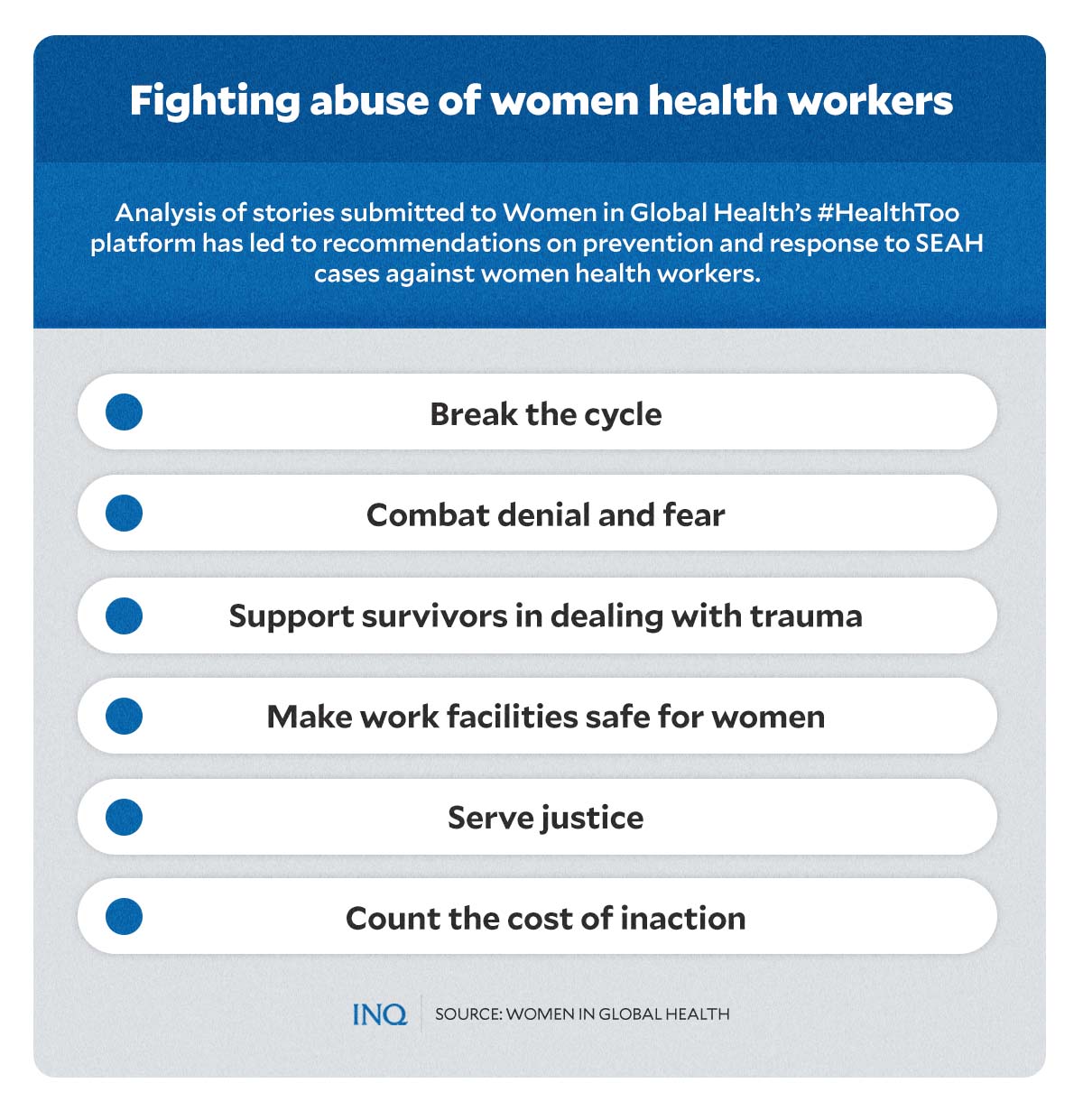
“In the absence of comprehensive data, Women in Global Health (WGH) launched the #HealthToo platform in 2022 for women in the health sector to lodge their stories of SEAH anonymously, shine a light on this largely invisible abuse and drive accountability,” the report stated.
WGH analyzed a total of 235 stories of SEAH from women in the health sector, submitted in 10 languages from 40 countries.
GRAPHIC Ed Lustan
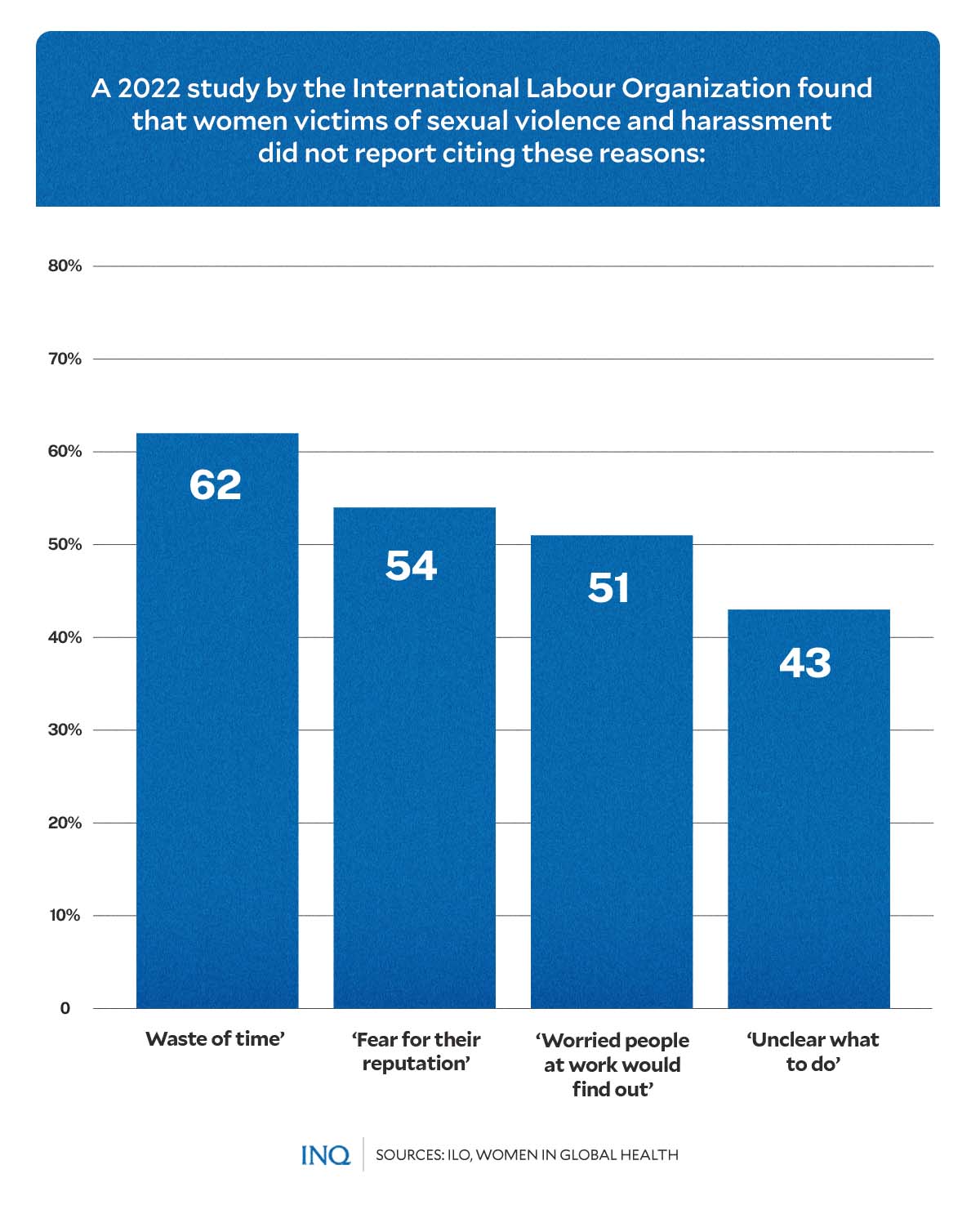
Four central themes emerged from those stories, which discussed the pattern of abuse, the type of incidents reported, the immediate and long-run trauma responses of victims, and why SEAH remains underreported among women health workers.
“The stories of the women health workers under #HealthToo, many harrowing to read, confirm earlier studies that SEAH is widespread in the health sector and the victims mainly women,” the WGH said.
Based on the stories it received, the organization concluded that across the globe, women health workers continue to experience work-related SEA, ranging from sexualized verbal abuse, sexual assault, and rape—all of which, WGH stressed, were unwanted and unprovoked by the victims.
Women in the health sector face different kinds of SEAH, from male co-workers, patients, and men in communities. Through the #HealthToo initiative, the organization also received a report of sexual harassment from a senior woman colleague.
Moreover, the analysis found that many male perpetrators appear to be serial abusers and are enabled by “silent bystanders.” This encourages a patriarchal culture that legitimizes, downplays, and perpetuates SEAH against women.
Alarmingly, WGH detailed that women’s experience of SEAH and trauma “is downplayed in the health sector and is even normalized.”
GRAPHIC Ed Lustan
Cases of SEAH in the health workforce, the report explained, hinder career progression and retention of women health workers—which, in turn, could impact morale, mental health, sickness absenteeism, and turnover—and could lead to staff shortages.
“SEAH improves the career progression opportunities for men in the health sector, creating a toxic working environment and reducing competition from women who may leave the role or the workforce,” said WGH.
Recognizing, identifying work-related abuse
The stories submitted by women in the health sector worldwide uncovered the varied nature of work-related SEAH.
Aside from cases of sexual assault and harassment, SEAH can also occur in the form of remarks and jokes—specifically sexist statements or pejorative remarks against an individual or a person’s gender “that are intended to reflect negatively on the individual.”
Sexual remarks can also be hard to separate from broader harassment. A story submitted by a nurse in Nepal showed what SEAH, masked as a joke or comment, looks and sounded like against women in the health sector.
“As I am working in the sector of sexual reproductive health and rights and I am vocal about the SRHR [sexual and reproductive health and rights] issues, some of the co-workers said, ‘I think you have all the experience for your future husband’,” the nurse said.
While women of every age can be targets for SEAH, #HealthToo stories highlighted how cases of workplace abuse among women occur and begin during their internships or studentships.
“Once, there was an attendant who was rubbing my back after I presented a patient to him. I felt so uncomfortable and embarrassed, but worse because I didn’t even know what to do as a resident,” a doctor from the US told WGH.
Another type of SEAH in the health workforce involves threats, retaliation, and abuse of power. Stories depicted how senior doctors or sector members used their position against women health workers to exploit them.
“He told me that I need to show him a good night-life in Nairobi. When I said no, he said, ‘How can we work together with this attitude of yours? It means you don’t want your promotion that much, which I can give you in 5 minutes.’ I still said no,” a Kenyan health administrator said.
“Then, after a couple of days, he informed me that I didn’t qualify for the role and that I had performed poorly over the past couple of months.”
Aside from abusers who hold influential positions in the workplace or have higher social statuses—making them superior to the victims—abusers can also be found outside the health sectors.
According to WGH, women health workers experience abuse and harassment from “male senior colleagues to male hospital drivers, male police, male health officers, male international health representatives, male teachers, male interns, male nurses, male patients.”
Moreover, while women are typically the victims of SEAH inflicted by male perpetrators, there are also instances where women abuse their power.
Gender inequity in health workforce
According to WGH, gender inequities in the health workforce increases the risk of SEAH for women—where women are marginalized in leadership, earn less than men on average, and are in less powerful roles.
Data showed that women hold only 25 percent of senior leadership roles in the health sector. This creates an enabling environment for SEAH, with a “pattern of men in higher status positions abusing power to coerce and force female employees into unwanted sexual contact in a cycle of ‘grooming,’ threats and retaliation.”
A working paper published in 2019 by WHO detailed that an average gender pay gap of around 28 percent exists in the health workforce. Once occupation and working hours are accounted for, the gender pay gap is 11 percent.
It also stressed that women are less likely than men to work full-time in the health and social sector.
“The hierarchical nature of medicine, status differences between professions, and clustering of women in lower status, lower paid and even unpaid roles, all leave women more vulnerable to abuse,” WGH explained.
“Women’s concentration in patient-facing roles, such as community health workers and nursing, brings them into more contact with patients and their visitors, who can be perpetrators,” it added.
“Many stories describe sexist behavior that belittles and demeans women, motivated by reinforcing power differentials and stereotypes of women’s subordinate position, and less by sexual desire.”
(Next: Patterns of work-related SEAH, why they remain underreported, what should be done.)
TSB
RELATED STORIES
End pandemic of violence against women
Gender-based violence: A disease more pervasive than COVID