‘Financial toxicity’ hurting PH cancer patients

INQUIRER.net COMPOSITE / Jerome Cristobal
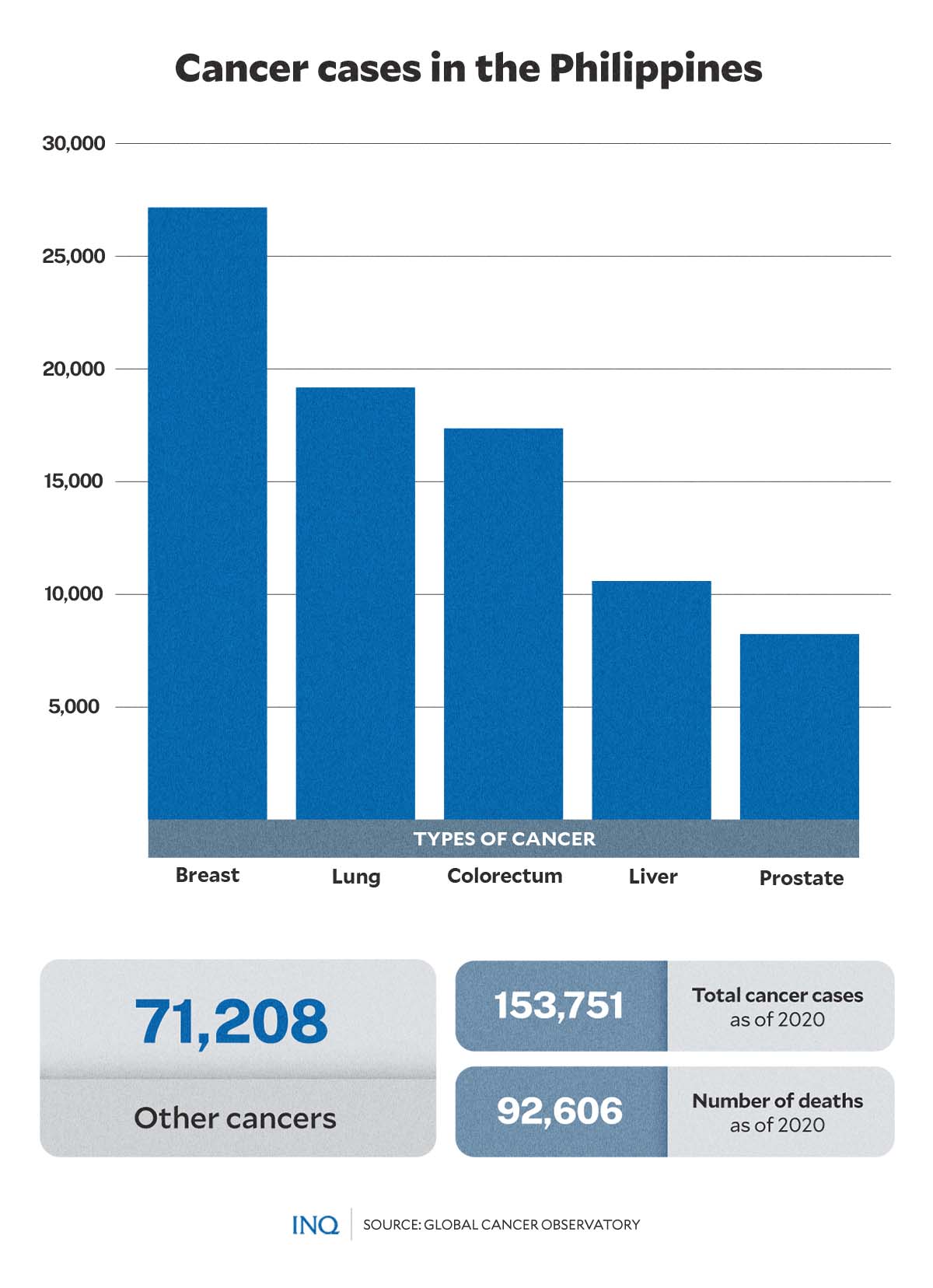
MANILA, Philippines—Estimates by the Global Cancer Observatory (Globocan) showed that 153,751 Filipinos suffer from various types of cancer as of 2020. Among these were 27,163 breast cancer patients, 19,180 lung cancer patients, and 17,364 colorectum cancer patients.
Several public health mechanisms supporting cancer control services are being implemented, including early screening and detection procedures, hospitalization benefits, and access to free cancer medication which are currently being offered for patients in the Philippines.
However, out-of-pocket expenditures in cancer care remain high among Filipino cancer patients, with medical costs of up to P100,000 per chemotherapy session.
GRAPHIC: Ed Lustan
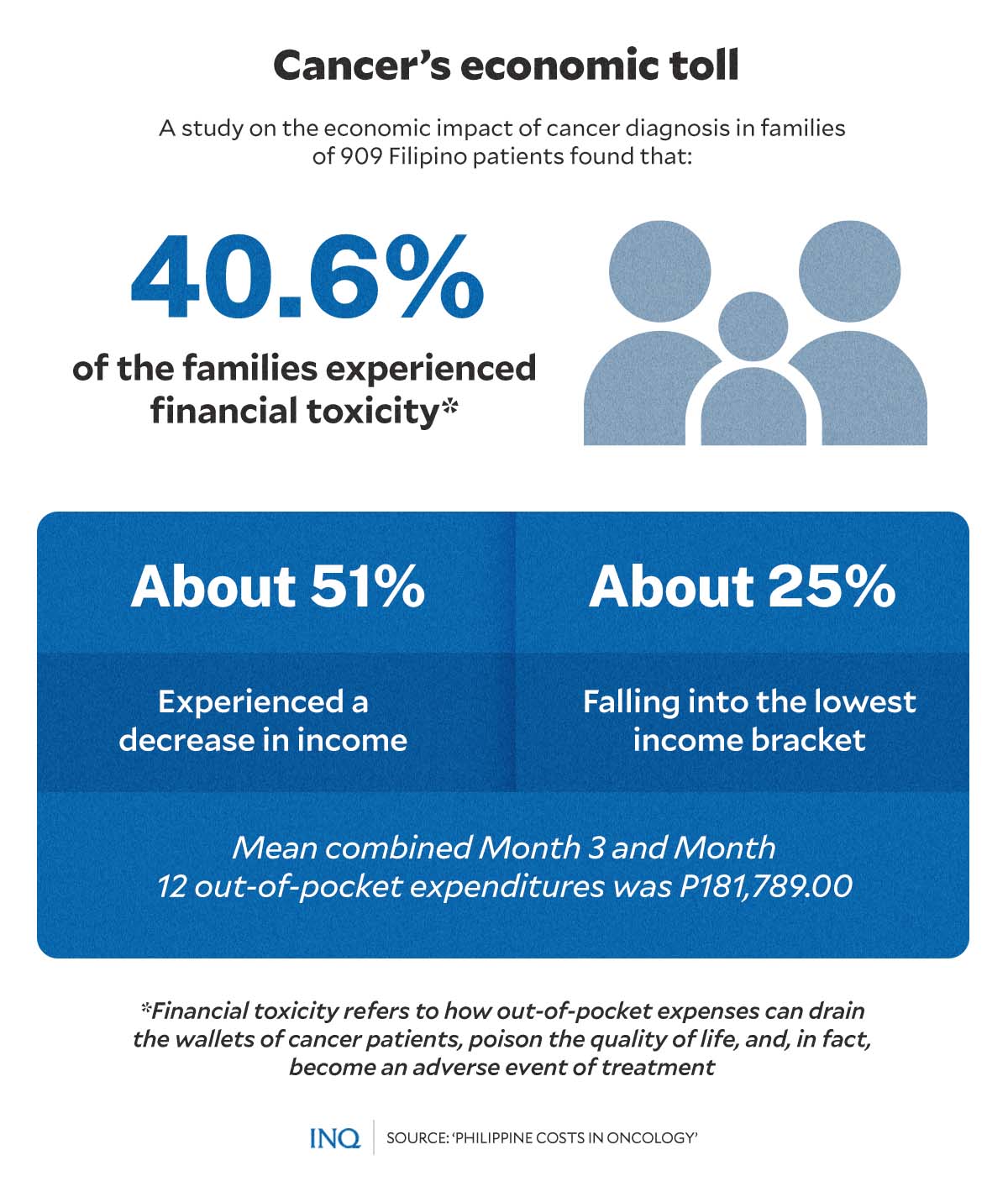
A study published in 2018 in Acta Medica Philippina—a peer-reviewed general medical and health science journal published by the University of the Philippines (UP)—highlighted the economic impact of cancer diagnosis in families.
The study, which analyzed 909 cancer patients in the Philippines, found that 40.6 percent of cancer patients’ families experienced financial toxicity—or financial problems—due to the high cost of medical care.
The researchers also found that the mean combined out-of-pocket expenses of respondents at 3 and 12 months after diagnosis amounted to P181,789.00.
Alleged graft, malversation of funds
But a complaint filed at the Office of the Ombudsman by a Department of Health (DOH) official accused top department officials of misappropriating cancer funds.
In the complaint, Dr. Clarito Cairo Jr., program manager of the DOH’s cancer control division under the Disease Prevention and Control Bureau, said the funds for cancer had been sub-allotted to only 20 access sites instead of 30 which is “a grave disservice to many cancer patients.”
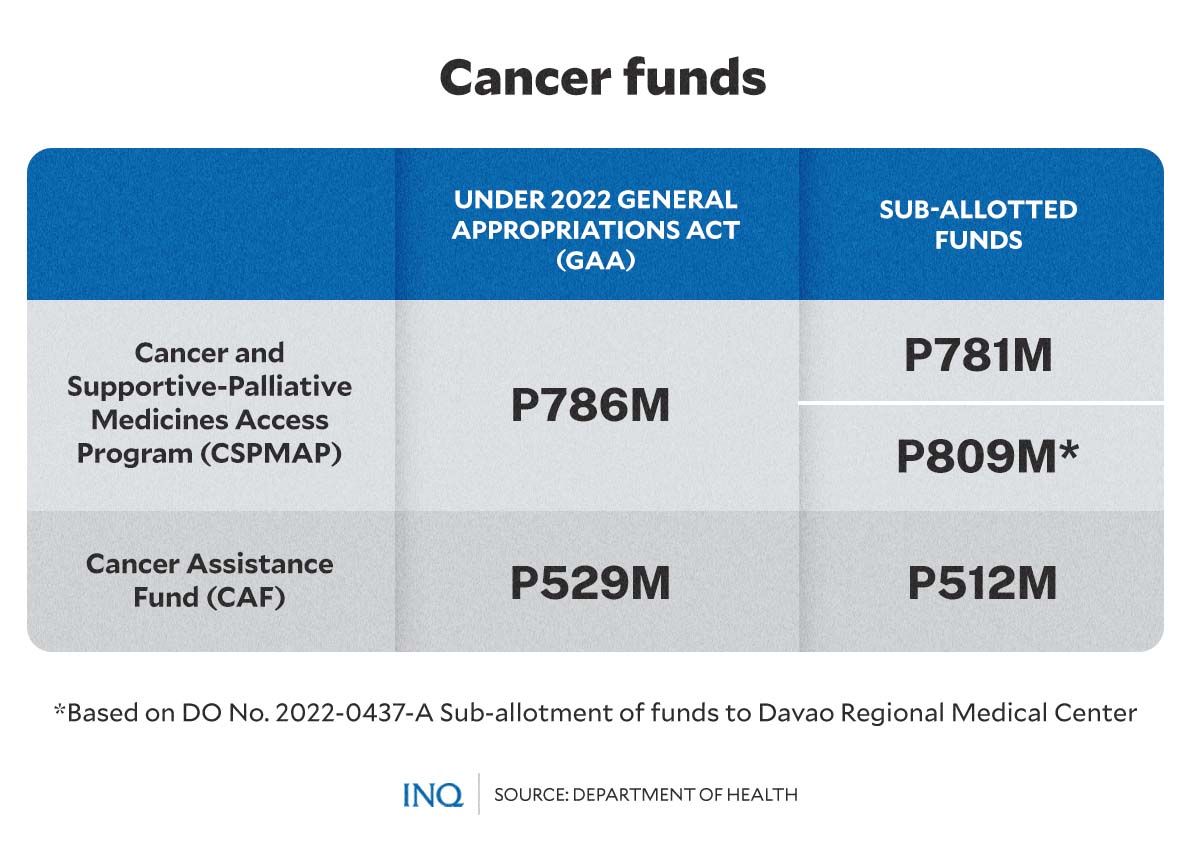
The funds were for the DOH’s Cancer and Supportive-Palliative Medicines Access Program (CSPMAP) which provides free medicines—supportive and palliative—for patients with different types of cancer.
GRAPHIC: Ed Lustan
Some of the types of cancer covered by CSPMAP are breast, childhood, lung, prostate, bladder, kidney, blood, head, neck, thyroid, gynecologic and gastrointestinal.
READ: DOH exec includes OIC in raps over cancer funds
In a TV interview, Cairo said the pooled procurement of cancer medicines was preferable as only “one entity”—or the central DOH office—would purchase medicines for all access sites. He said centralization was more advantageous in this case.
“Among the advantages [are] reduced corruption, more efficient procurement processes, increased access to medicines, and cost savings,” he said.
“Those advantages, we cannot see [those] in the sub-allotment of funds in the access sites because different access sites have different turnaround times for their procurement. The volume will decrease, and unit cost will increase,” he added.
Cairo also claimed there had been undue preference for a more costly brand of cancer drug which strayed from medicine prices under the 2022 edition of the Drug Price Reference Index of the DOH.
Experts, specialists back DOH
In response to the complaint, Health Undersecretary Maria Rosario Vergeire, who is acting DOH chief, explained that all processes involved in the agency’s cancer programs were implemented with transparency.
“I want to give the public assurance that everything that we are doing in the process for the agency’s programs, specifically in the cancer funds, is aboveboard,” she said at a media forum.
She added that everything “was done in a transparent manner” and that the DOH consulted experts in the National Integrated Cancer Control Council (NICC)—the highest policy-making body for cancer control in the Philippines—for direction and decisions.
In a statement, several non-officio members of NICC attested that “all stakeholders that the P786-M fund in question is all accounted for.”
“The decision to sub-allot/transfer the funds to the hospitals was discussed and agreed upon by the council due to the exigency of providing medicines to patients and to prevent and address gaps in patient treatment,” they said, referring to the NICC.
A separate statement released by 20 public hospitals—all of which serve as access sites for the CSPMAP—assured that over P809 million had been allocated to them and “have been used efficiently.”
The state-run hospitals added that the funds continued to be used to procure cancer medicines for patients.
The DOH clarified that the hospitals allegedly excluded from receiving funds “were actually provided cancer medicines and cancer assistance funds which can be used for diagnostics, treatment, and other needed support of cancer patients.”
READ: More funding, assistance bring cancer patients closer to recovery
Decentralizing specialized health services
In the complaint, Cairo said that one of the respondents “should have known better that pooled procurement is the most cost-efficient mode for the costly cancer medicines.”
He added that had pooled procurement been used for cancer medicines in 2022, more patients enrolled in CSPMAP in 2021 across 31 access sites would have continued their necessary treatment.
GRAPHIC: Ed Lustan
A health expert, who preferred to be an anonymous source, echoed Cairo’s claims.
“Outcome of treatment in cancer depends heavily on timely administration of service, especially chemotherapy. If you stop the supply of drugs, then you put [the patients’] lives in danger,” the source told INQUIRER.net.
While Cairo cited a systemic review that analyzed the advantages of pooled procurement, several studies in favor of more decentralization in the health sector argued for its benefits.
These advantages include “empowerment of local authorities to make decisions on their own, reducing levels of bureaucracy to achieve efficiency, better matching of health services with local priorities, promoting innovations in service delivery that address local needs, and enhancing stakeholder participation in decision-making.”
Other systematic reviews examined the effectiveness of decentralizing health service delivery in treating MDR-TB patients—where treatment success was higher—and in providing anti-retroviral therapy for HIV patients—which showed that the loss to followup was less.
Both studies recommended further studies to explore the effectiveness of decentralizing treatment in various settings.
A synthesis report by the World Health Organization’s Department of Health Systems, Governance, and Financing (WHO/HGF) and ThinkWell published last year likewise analyzed the interplay among decentralization, public financial management (PFM), and health financing through case studies performed on seven countries, including the Philippines.
The synthesis report noted the “considerable need for further research on the interplay among decentralization, PFM, and health financing.”
An editorial published by the Philippine Daily Inquirer (PDI) stressed that the government needed to decentralize specialized health services from Metro Manila to the provinces.
“This is mandated under the Philippine Health Facility Development Plan 2020-2040, which envisions the establishment of health care facilities throughout the country,” the editorial read.